
ICD-10 and CPT Codes: Answers to Questions About COVID-19 Visits
February 23, 2022
In the last two years, we’ve seen a lot of change. Among the most frustrating are the continual changes to the rules around coding and documentation — which had remained the same for 25 years. This creates ongoing confusion for clinics, bottlenecking processes and creating challenges in getting paid.
Experity’s RCM Compliance manager, Phyllis Dobberstein, hosted a webinar to clarify COVID-19 coding and how to prevent resulting bottlenecks in the future. Kick Off 2022 with Coding Confidence is informative from start to finish, but below we address three of the most common questions being asked.
Please note that this information is accurate as of February 22, 2022, and may not apply in all situations. Refer to full discloser at the end of this article.
Read on to learn about proper reimbursement, new ICD-10 codes, and in-house CPT codes.
Like most things COVID, this isn’t a completely straightforward answer. But Dobberstein was able to provide some clear direction for us.
For starters, two acts — the Families First Coronavirus Response Act (FFCRA;) and the Coronavirus Aid, Relief, and Economic Security Act (CARES) — require insurance to cover diagnostic testing without cost sharing.
So at the federal level, yes. Insurance plans are required to cover diagnostic testing. For clarity:
Diagnostic = used for treatment
Patients are symptomatic or asymptomatic but exposed
However, screenings may not be covered. Antibody testing may be covered with cost sharing. But coverage requirements can change from state to state. In October, California passed a senate bill adding language to the Knox-Keene Act that requires screenings to be covered. So as is a best practice for all things COVID, research the rules in your state.
Regardless, whether the visit is covered revolves around diagnoses and why the patient came in for a visit. In contrast to diagnosis:
Screening – used for administrative purposes (e.g., screening for travel)
Patients are asymptomatic and have not been exposed
Given this, Dobberstein cautions we be careful using the word “screening” in the medical record when the patient is truly presenting for diagnostic. This will help you avoid misunderstandings. Additionally, some individual payers may not even want screenings sent to them. In this case, you’d have to collect from the patients directly, so it’s important to check with the payers.
Remember: if your claim isn’t clean, the chance of collecting is reduced significantly.
For more information about how to use specific ICD-10 and other codes, including the latest pertaining to late-effect COVID, download the on-demand webinar >>
There are some new codes coming in April of 2022 to report under-immunization for COVID-19 status.
| Code | Details |
| ICD-10: Z28.310 | Unvaccinated for COVID-19 |
| ICD-10: Z28.311 | Partially vaccinated for COVID-19 |
| ICD-10: Z28.39 | Other under-immunization status |
However, Dobberstein speculates that these codes were created for hospitals that get paid on a DRG (diagnosis-related group.) A patient that is vaccinated will require fewer resources than a patient that is unvaccinated. If that is the purpose for these codes, you wouldn’t necessarily be using them for an urgent care visit. In any case, these codes should not be used at all until April 1, 2022.
When it comes to lab codes, in-house labs have been especially confusing in our journey with COVID-19. However, the AMA (American Medical Association) provided clarification in March of 2021 that has remained consistent since.
Any lab, any test, counts once per each unique CPT code. No matter the number of times you’re billing that CPT code, it’s still one unique CPT code, or one point.
For example, if you’re doing flu and billing for Influenza A and Influenza B, it’s the exact same CPT code. You bill it twice, but you only count it once.
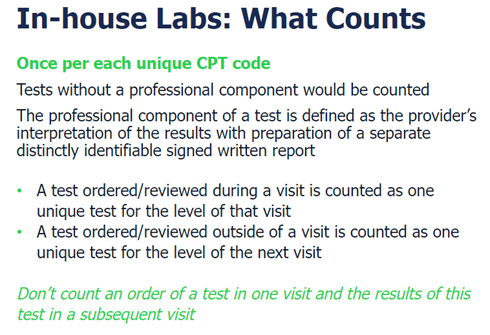
The only thing you can count are tests without a professional component performed in the office. Those are your labs, which you’re always going to count. A professional component is when you have an interpretation with some type of report — interpretation of the x-ray or EKG, for example. We count labs because they don’t have a professional component, or interpretation element. However, you can count them ONCE. A test reviewed during a visit is counted one time. You cannot subsequently count it on another visit while it was being reviewed.
If it helps, here is the slide summarizing this information:
These are confusing times for urgent care coding. We want you to feel confident about getting paid. We created a downloadable cheat sheet based on that blog here (which is current as of 2/17/22.)
For a more conversational explanation of coding, Dobberstein dives into diagnoses codes, lab codes, E/M coding, and suggestions for 2022 in Kick Off 2022 with Coding Confidence.
DISCLAIMER: While this page represents our best efforts to provide you with guidance and useful advice, we cannot guarantee that third-party or government payers will recognize and accept our recommendations. The analysis of any medical or billing coding question is dependent upon numerous specific facts – including the factual situations present related to patients, the professionals, the medical services provided and the medical record documentation.
In addition, laws and regulations and insurance and payer policies are subject to change. The information that has been accurately provided in the past could change depending upon changes in such laws or regulations.
The information provided is intended to provide general guidance. It is not intended to serve as medical, health, legal or financial advice or as a substitute for professional advice from a healthcare consultant, legal counsel or another professional advisor
In no event, will Experity be liable for any loss or damage including without limitation, indirect or consequential loss or damage, or any loss or damage whatsoever arising from loss of data or profits arising out of, or in connection with, the use of this guidance.

Join over 20,000 healthcare professionals who receive our monthly newsletter.

Join over 20,000 healthcare professionals who receive our monthly newsletter.


